Correct understanding of the geometry of the glenoid (the socket of the shoulder joint) is key to successful planning of
shoulder replacement surgery. This surgery typically involves placing an implant in the shoulder joint to restore joint
function. The most relevant geometry is the glenoid version, which is the angular orientation of the glenoid surface
relative to the long axis of the scapula in the horizontal (axial) plane. However, measuring the glenoid version is not
straightforward and there are multiple measurement methods in the literature and used in commercial planning
software.
Glenoid version can be computed from 2D radiographs or from 3D CT scans. The use of radiographs for glenoid
measurement has been shown to be less reliable that CT based methods,18 so most modern approaches use CT scans for
glenoid version measurement. Methods using CT scans can be divided into 2D methods that use a single axial slice to
estimate glenoid version and 3D methods that use landmark points in multiple slices. 2D methods have
been shown to be more susceptible to positional variance,5 however there is not as yet an agreed single
method for glenoid version measurement. There are many papers comparing the use of different methods for
measuring glenoid version or proposing new methods.4,7,24,25 Different methods are also implemented by
implant vendors and commercial software suppliers1–3 however, the exact methods used in each case are not
published.
There is a need therefore for reliable open source implementations of the various methods for measuring glenoid
version to enable further research comparing the methods. We have developed SciKit-SurgeryGlenoid to
meet this need and herein present early results of SciKit-SurgeryGlenoid’s use on retrospectively gathered
data.
2.
SciKit-SurgeryGlenoid currently implements two 3D methods; the two-plane method described by Ganapathi et al.13
and the 3D corrected Friedman method described by Budge et al.6 SciKit-SurgeryGlenoid also implements two 2D
methods; Friedman’s method11 and the vault method described by Matsumura et al.16 Each implementation can be
accessed via a command line application which takes as input a file describing the anatomical position of the required
landmark points.
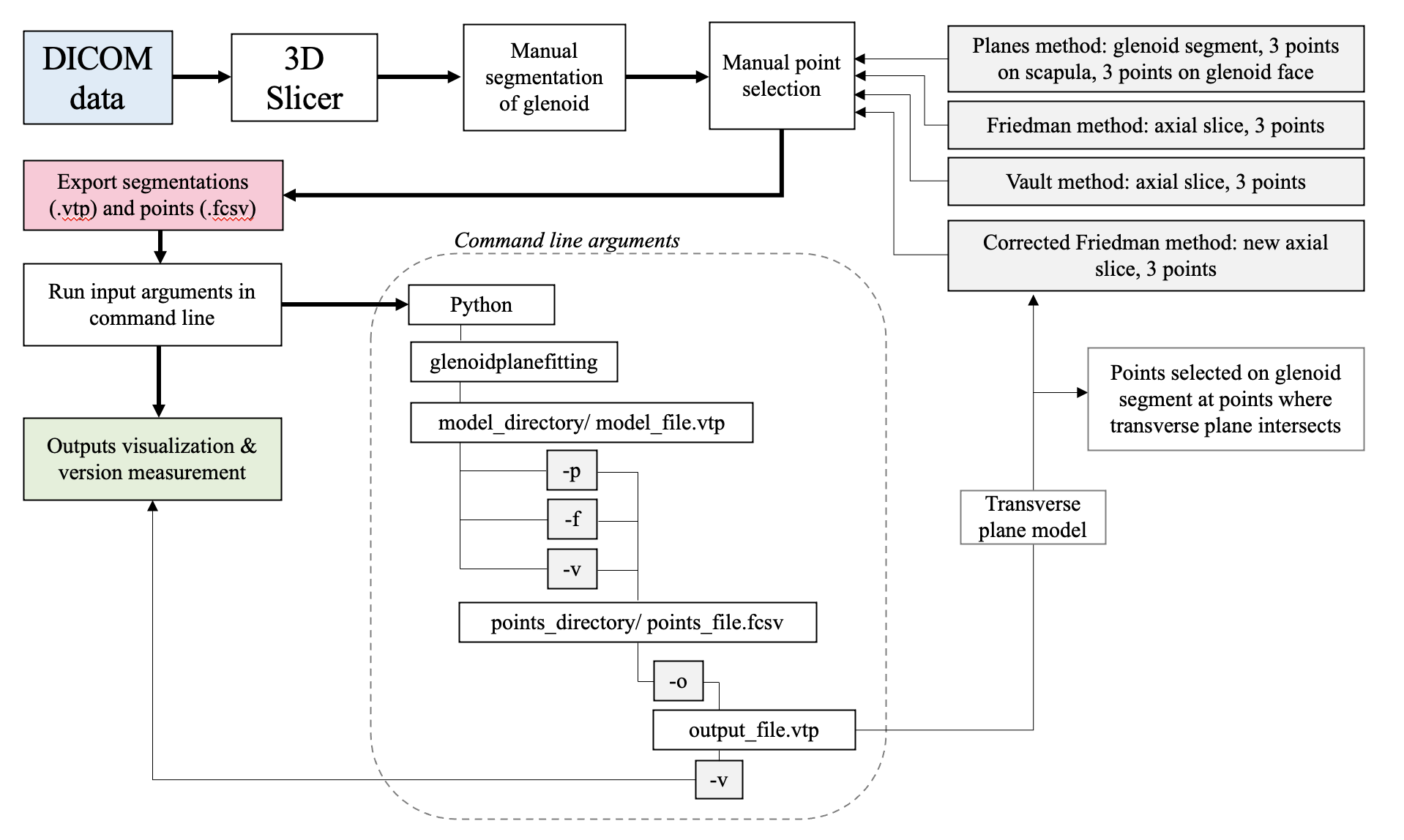
Although the longer term aim is to automate the identification of landmark points, SciKit-SurgeryGlenoid currently
requires the landmark points to be manually identified. Figure 1 gives a graphical description of the work flow we
used.
The selection of the different landmark points for each method and calculations of version measurements were done
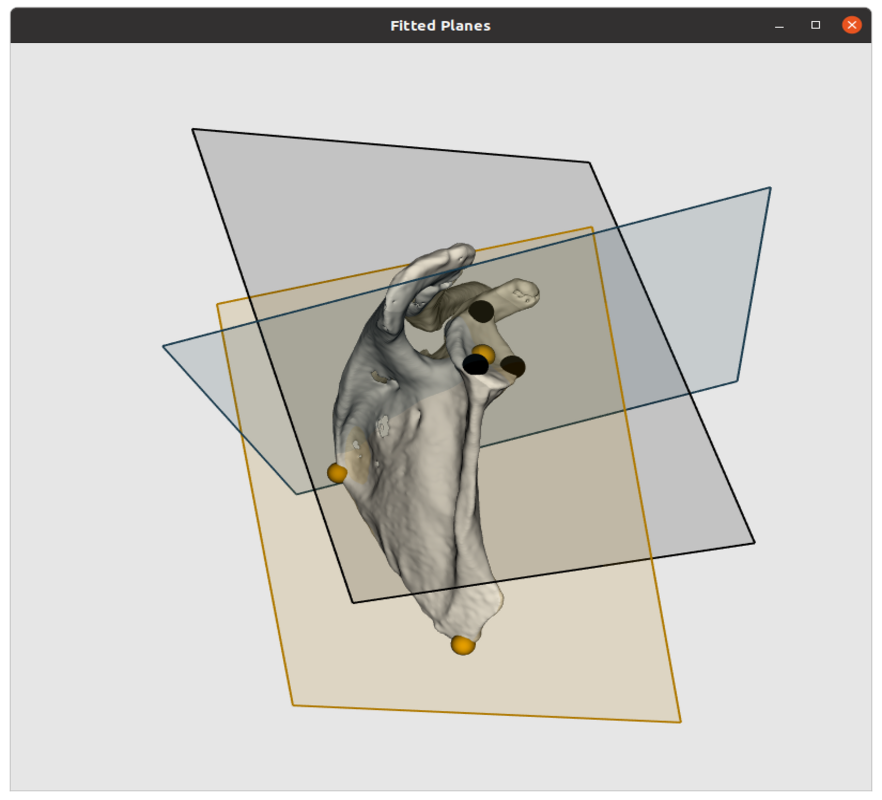
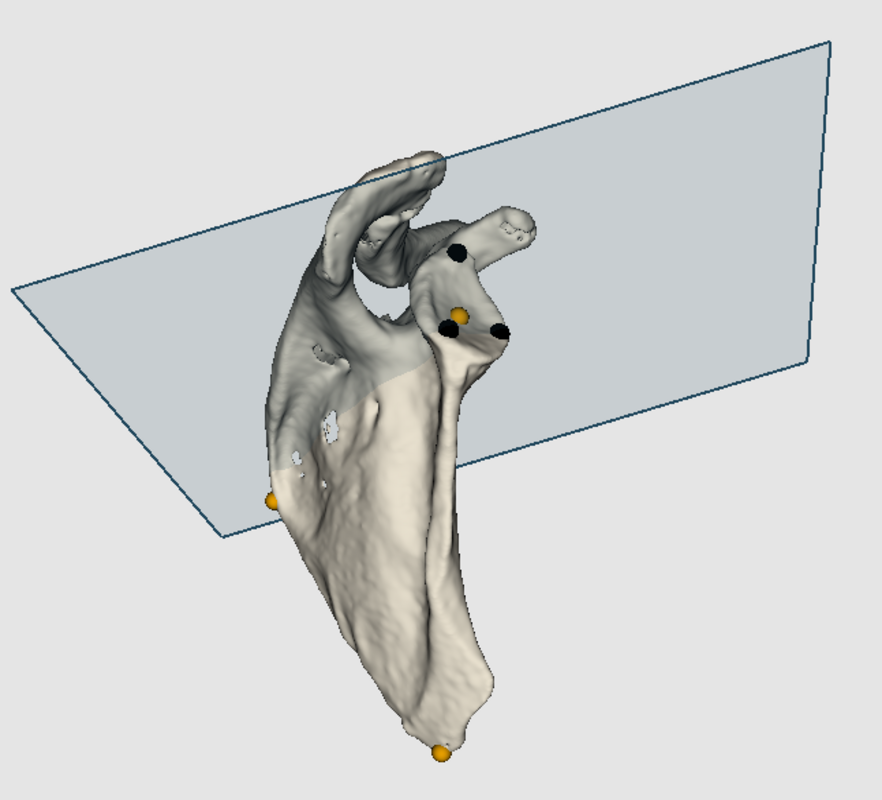
as follows. For the two-plane method, 3 points were chosen for each plane. For the glenoid fossa plane the
points selected were near the rim, one at the superior pole of the glenoid and two on the lower third of the
glenoid anteriorly and posteriorly (black points on figure 2a). For the scapula plane, the 3 points included
one at the center of the glenoid, another at the medial border of the scapula where the scapular spine
intersects the scapular body, and a third at the inferior tip of the scapula (orange points on figure 2a). The
glenoid version was then calculated as the angle between the plane of the glenoid fossa and the plane of the
scapula.
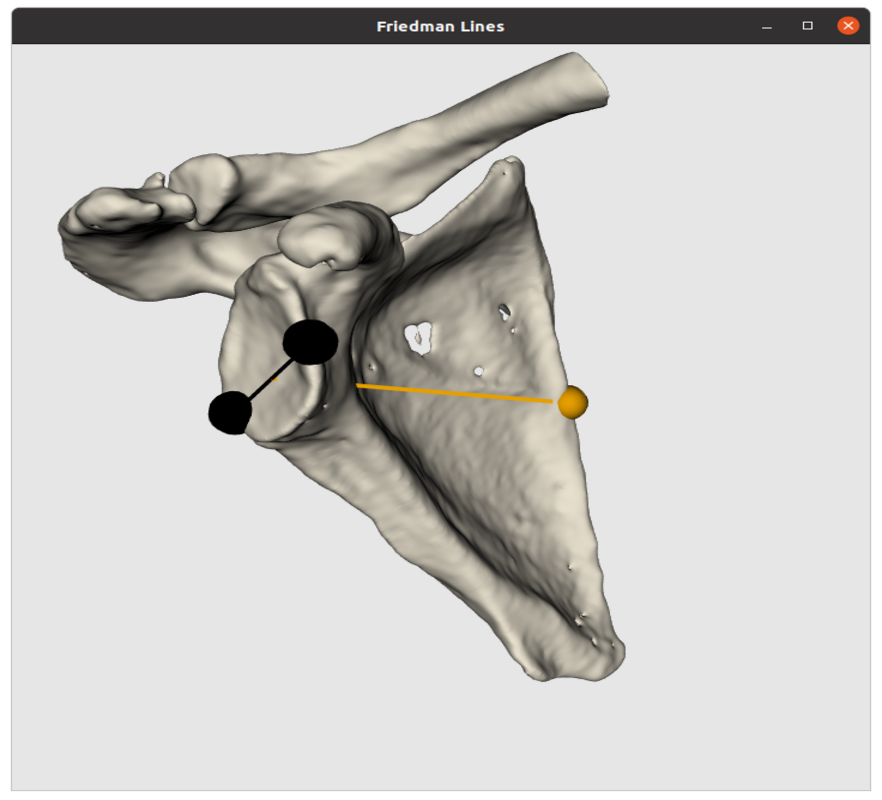
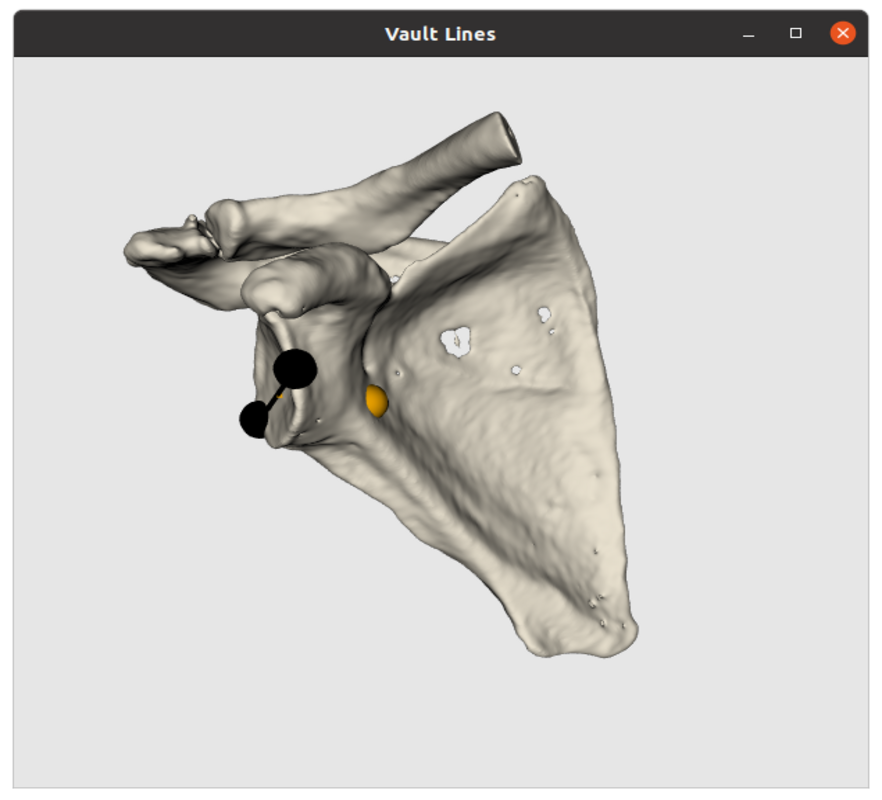
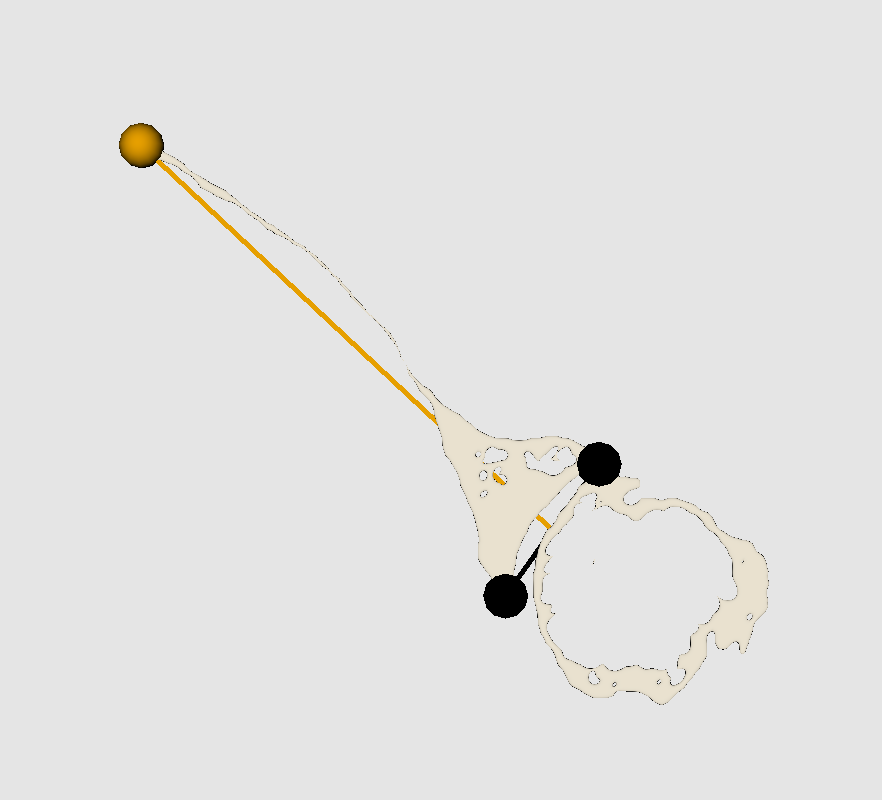
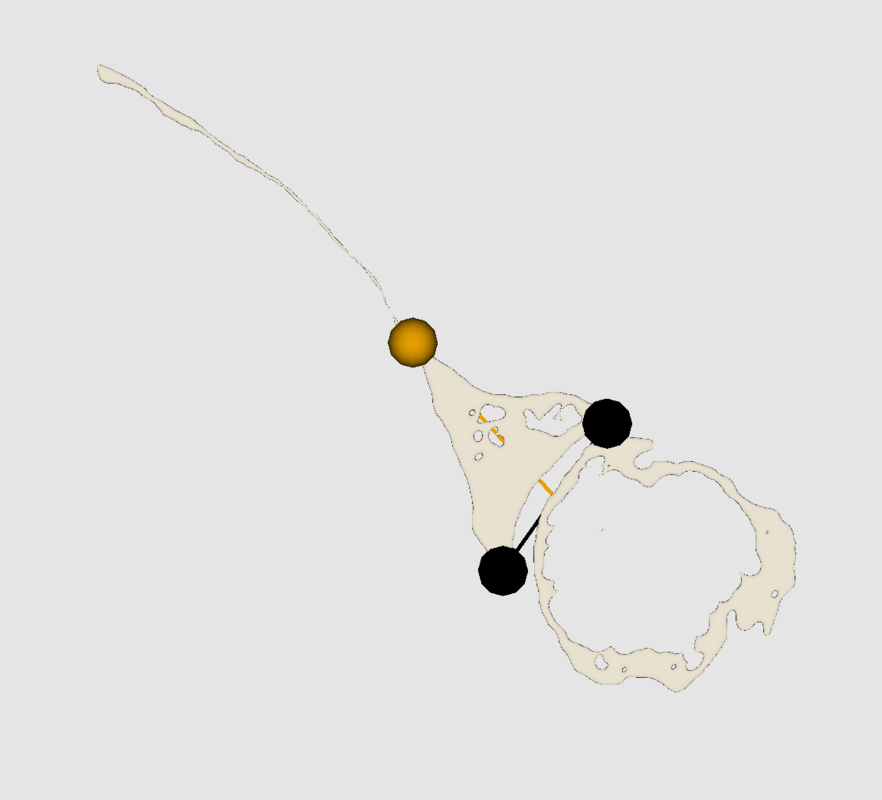
For the Friedman and vault method 3 points were chosen to form 2 lines. Both require the same two points at the
edges of the glenoid fossa anteriorly and posteriorly (black points on 2b and 2c). For the Friedman method the third
point was selected at the tip of the scapula, while for the vault method it was at the tip of the scapular vault. The point
selection was done on a 2D axial slice (see 2e and 2f). Therefore, slice choice is important and in this case was
selected as the axial slice at which the coracoid process is no longer visible. The Friedman line was formed
with the medial point on the scapula and the midpoint between the glenoid fossa points, while the vault
line was formed with the tip of the scapular vault and the same midpoint. The second line was formed
across the glenoid fossa in both methods. The version was then calculated as the angle between the two
lines.
The corrected Friedman method requires the same anatomical landmark points as the conventional Friedman
method, but on a corrected axial plane. This plane (blue plane in 2a) should be perpendicular to the scapular plane
which is formed by the same 3 points as the scapular plane for the two-plane method (black plane in 2a). The new
transverse scapular plane (blue plane in 2d) was used to generate a new 2D image slice on which the same conventional
Friedman landmark points were selected.
2.2
SciKit-Surgery is made up of multiple Python libraries that can be assembled into varied applications for research in
image guided surgery. Some current examples of SciKit-Surgery’s use include clinical guidance systems,20 research
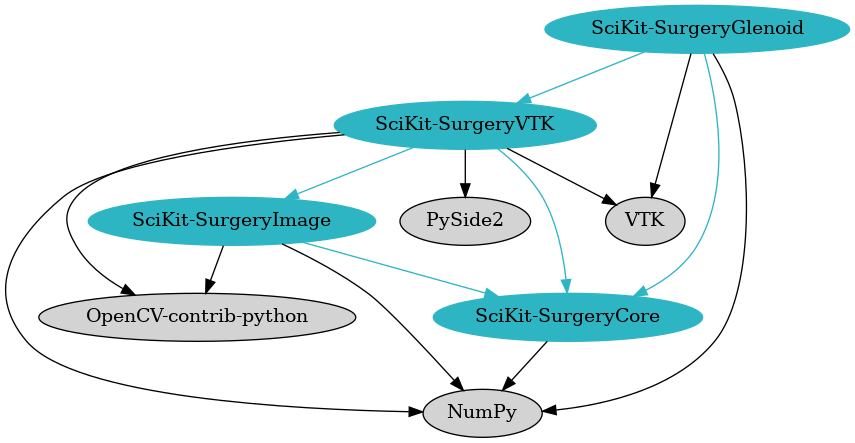
platforms for registration26 and ultrasound simulators.28 Figure 3 shows the immediate dependencies of
SciKit-SurgeryGlenoid. The most significant dependencies are NumPy14 which is used for the version
calculation, and VTK21 which is used for visualising the results. SciKit-SurgeryCore provides configuration
helpers for the user interface. SciKit-SurgeryVTK provides some helpful loaders and shape primitives, but it
may be useful to remove this dependency in the future as it would significantly simplify the dependency
graph.
We tested the performance of SciKit-SurgeryGlenoid on 10 anonymised CT scans from patients eligible for shoulder
replacement surgery. For each CT scan we performed segmentation and landmark annotation using 3DSlicer15 and
processed the resulting segmentation using SciKit-SurgeryGlenoid.
Statistical analysis was performed using GraphPad Prism software version 8.0 for Mac
. The
mean and standard deviation of each method was calculated and compared. Our current clinical practice uses planning
software from DJO Surgical,2 so we compared the results from SciKit-SurgeryGlenoid with the results
from the DJO Surgical software. Pearson’s correlation coefficient was determined between the commercial
software and each method. A repeated measures ANOVA was performed to determine any significant
differences in version measurements between the methods. Significance level for all analyses was set at
0.05.
3.
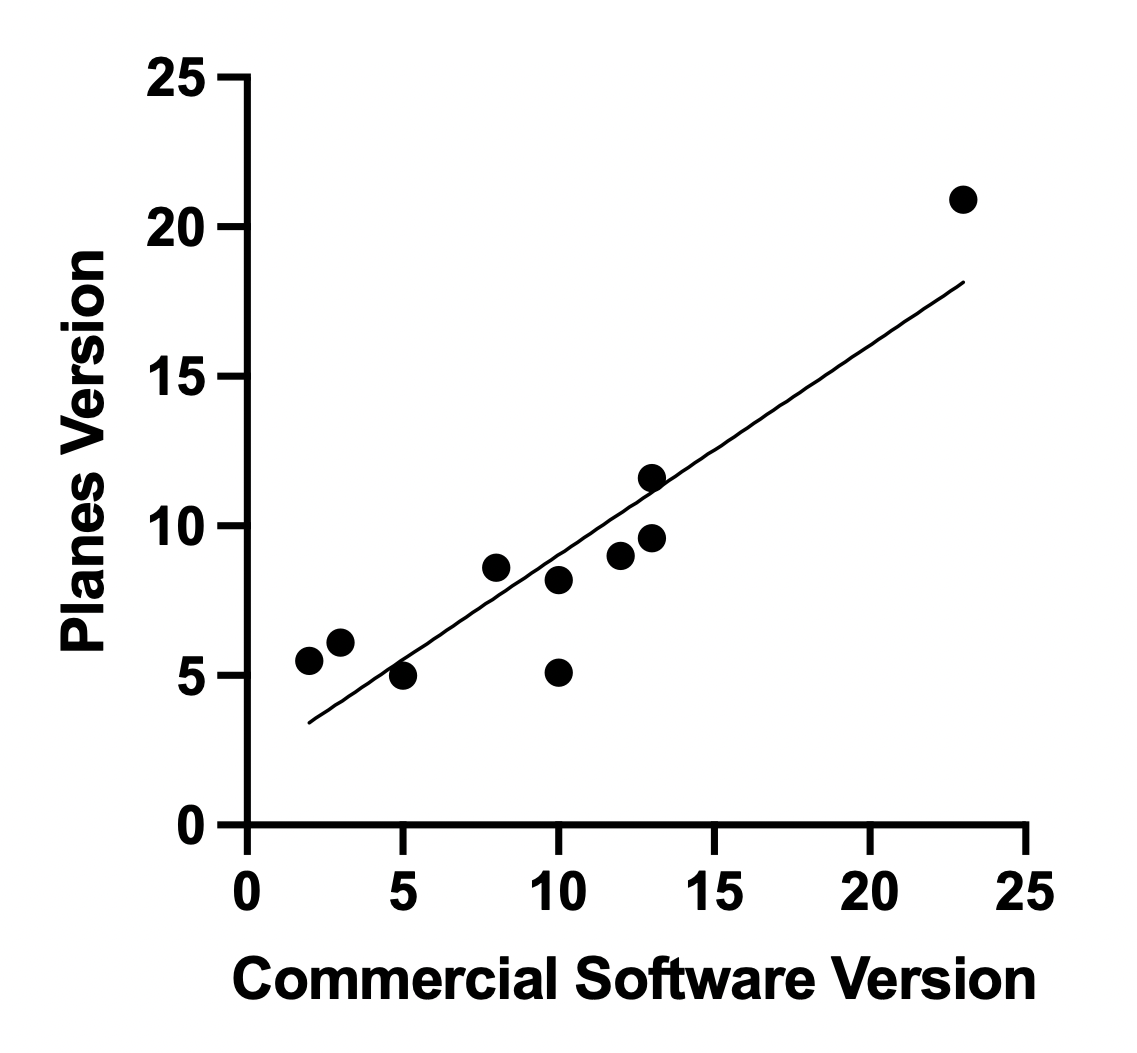
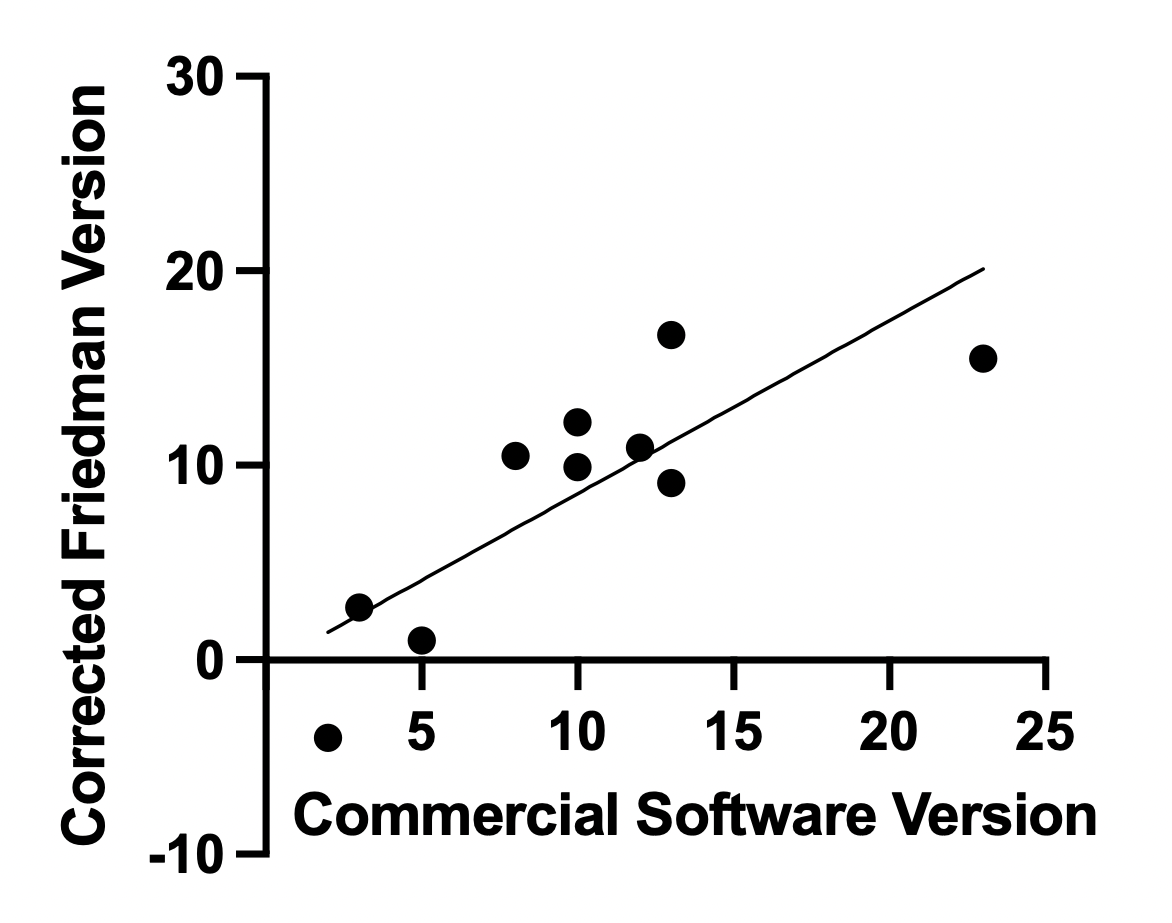
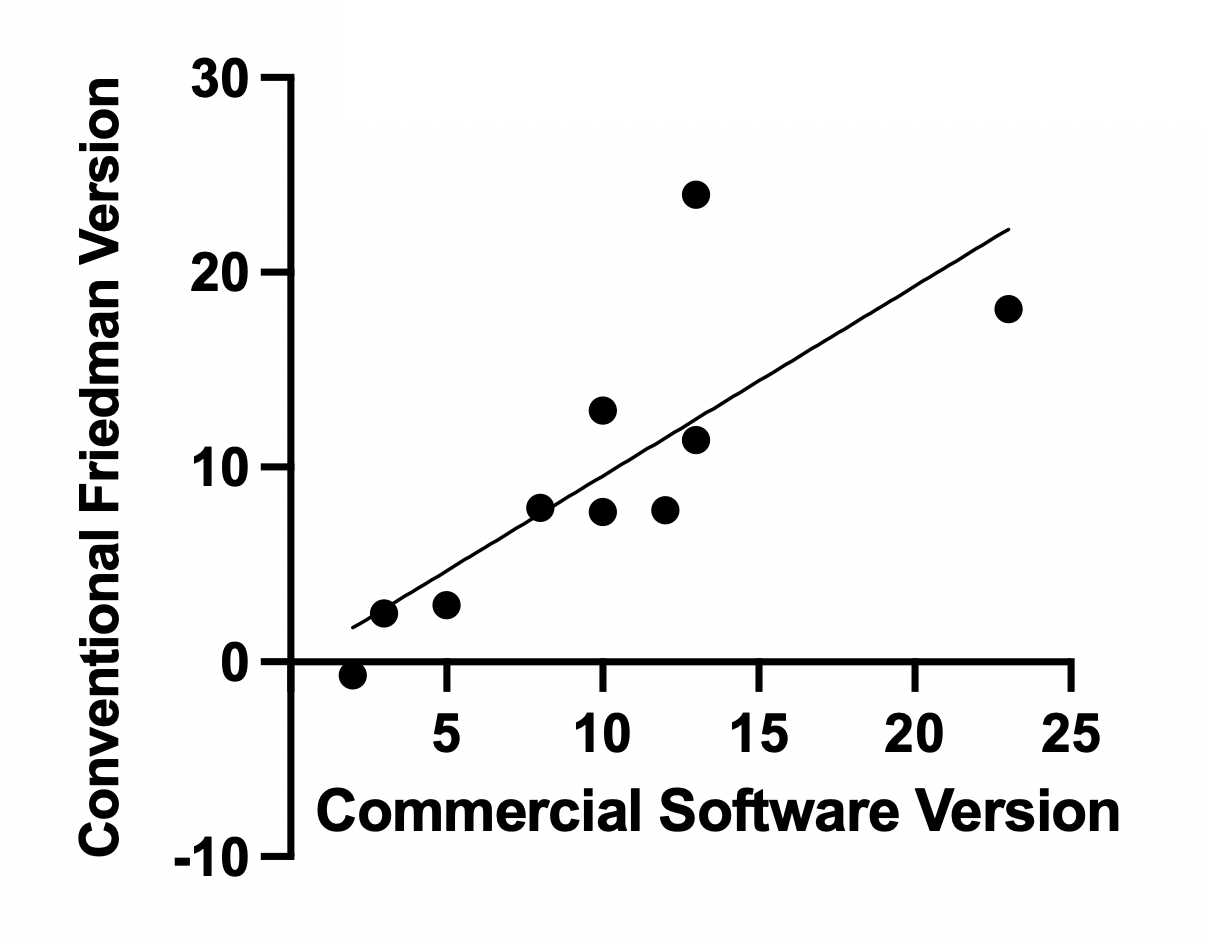
The measurements using these methods were also compared with version measurements on the same 10 patients
using a commercial software.2 The planes method (r = 0.90, p = 0.0004), corrected Friedman method (r = 0.83, p =
0.0034), and conventional Friedman method (r = 0.79, p = 0.0064) all showed significant correlation with the commercial
software. The vault method did not show significant correlation (r = 0.59, p = 0.074). The mean difference between the
methods were overall not significant (p > 0.05), except for the vault method (p = 0.03). Correlation plots are shown in
Figure 4.
There are several methods that have been proven to be accurate in preoperative measurement of the glenoid version.
Specifically, 3D methods have become the standard as they provide a higher accuracy accounting for the positional errors
during image acquisition (Budge et al.,6 Moineau et al.17). Testing the most common 2D and 3D methods using the
SciKit-SurgeryGlenoid toolkit allowed for an evaluation of its effectiveness in comparing these methods. The early results
presented are consistent with previously reported results (Matsumura et al.,16 Budge et al.,6 Ganapathi et
al.13).
While the mean version did not show any significant difference between most methods, this could be due to the small
sample size used in this case. However, it is notable that the 3D methods reveal slightly lower version means and
lower standard deviations which could prove significant when more scans are analysed with additional
observers.
From the Pearson correlation coefficient, significant correlation between the commercial software and 3 out
of the 4 methods was seen. The vault method showing little correlation with the commercial software
could be due to its much higher mean version value. The vault method tends to overestimate the glenoid
version as has been previously reported by several studies (Cunningham et al.,8 Matsumura et al.16).
The correlation tests prove however that there is good agreement between SciKit-SurgeryGlenoid and the
commercial software already in use, indicating accuracy and credibility of this toolkit. While this can be a
good indicator of reliability, further measurements using this software by different observers would be
needed to be able to test inter and intra observer reliability. However, SciKit-SurgeryGlenoid proves to be
promising in providing an unbiased way of comparing the many different methods available to measure glenoid
version.
Limitations of this initial testing of SciKit-SurgeryGlenoid include the small sample size used. A study with a wider
range of CT scans could reveal better understanding of the software’s reliability. Additionally, as points for each method
were selected manually, there are some inaccuracies that arise which could be better understood with repeated
measurements and multiple observers.
SciKit-SurgeryGlenoid provides a useful resource for shoulder arthroplasty. Future work could look at either automating
the segmentation process using state of the art registration algorithms12 to create a fully automatic pipeline, or at
integrating the library with 3DSlicer to create a “slicelet” based application, similar to our previous work23 in skull base
navigation.
This research was funded in whole, or in part, by the Wellcome Trust [203145Z/16/Z]. For the purpose of Open Access,
the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this
submission.
This work is supported by the Wellcome/EPSRC Centre for Interventional and Surgical Sciences (WEISS)
[203145Z/16/Z].
1. Blueprint 3D planning software. https://www.wright.com/blueprint-3d-planning-psi-system.
Accessed: 2021-07-27
2. DJO surgical. https://www.djoglobal.com/our-brands/djo-surgical. Accessed: 2021-08-04
3. Exactech equinox. https://www.exac.com/extremities/equinoxe-platform-system/. Accessed:
2021-07-27
4. Boileau, P., Cheval, D., Gauci, M.O., Holzer, N., Chaoui, J., Walch, G.: Automated three-dimensional
measurement of glenoid version and inclination in arthritic shoulders. The Journal of bone and joint surgery.
American volume 100(1), 57—65 (2018). URL https://doi.org/10.2106/jbjs.16.01122
5. Bryce, C.D., Davison, A.C., Lewis, G.S., Wang, L., Flemming, D.J., Armstrong, A.D.: Two-dimensional
glenoid version measurements vary with coronal and sagittal scapular rotation. JBJS 92(3), 692–699 (2010)
6. Budge, M.D., Lewis, G.S., Schaefer, E., Coquia, S., Flemming, D.J., Armstrong, A.D.: Comparison
of standard two-dimensional and three-dimensional corrected glenoid version measurements. Journal of
Shoulder and Elbow Surgery 20(4), 577–583 (2011). URL https://doi.org/10.1016/j.jse.2010.11.003
7. Choi, C.H., Kim, H.C., Kang, D., Kim, J.Y.: Comparative study of glenoid version and inclination
using two-dimensional images from computed tomography and three-dimensional reconstructed bone models.
Clinics in shoulder and elbow 23(3), 119—124 (2020). URL https://doi.org/10.5397/cise.2020.00220
8. Cunningham, G., Freebody, J., Smith, M.M., Taha, M.E., Young, A.A., Cass, B., Giuffre, B.:
Comparative analysis of 2 glenoid version measurement methods in variable axial slices on 3-dimensionally
reconstructed computed tomography scans. Journal of shoulder and elbow surgery 27(10), 1809—1815
(2018). URL https://doi.org/10.1016/j.jse.2018.03.016
9. Doel, T., Thompson, S., Dowrick, T., Ahmad, M., Clarkson, M.: Python template (2022). URL
https://doi.org/10.5281/zenodo.5879146
10. Dowrick, T., Ahmad, M., Thompson, S., Hetherington, J., Cooper, J., Clarkson,
M.: Cmakecatchtemplate: A c++ template project. Journal of Open Research Software 9(1) (2021). URL
http://doi.org/10.5334/jors.319
11. Friedman, R., Hawthorne, K., Genez, B.: The use of computerized tomography in the measurement of
glenoid version. The Journal of bone and joint surgery. American volume 74(7), 1032—1037 (1992). URL
http://europepmc.org/abstract/MED/1522089
12. Fu, Y., Brown, N.M., Saeed, S.U., Casamitjana, A., c. Baum, Z.M., Delaunay, R., Yang, Q., Grimwood,
A., Min, Z., Blumberg, S.B., Iglesias, J.E., Barratt, D.C., Bonmati, E., Alexander, D.C., Clarkson, M.J.,
Vercauteren, T., Hu, Y.: Deepreg: a deep learning toolkit for medical image registration. Journal of Open
Source Software 5(55), 2705 (2020). URL https://doi.org/10.21105/joss.02705
13. Ganapathi, A., McCarron, J.A., Chen, X., Iannotti, J.P.: Predicting normal glenoid version from the
pathologic scapula: a comparison of 4 methods in 2- and 3-dimensional models. Journal of shoulder and
elbow surgery 20(2), 234—244 (2011). URL https://doi.org/10.1016/j.jse.2010.05.024
14. Harris, C.R., Millman, K.J., van der Walt, S.J., Gommers, R., Virtanen, P., Cournapeau, D., Wieser, E.,
Taylor, J., Berg, S., Smith, N.J., Kern, R., Picus, M., Hoyer, S., van Kerkwijk, M.H., Brett, M., Haldane, A.,
Fernández del Río, J., Wiebe, M., Peterson, P., Gérard-Marchant, P., Sheppard, K., Reddy, T., Weckesser,
W., Abbasi, H., Gohlke, C., Oliphant, T.E.: Array programming with NumPy. Nature 585, 357–362 (2020).
URL https://doi.org/10.1038/s41586-020-2649-2
15. Kikinis, R., Pieper, S.D., Vosburgh, K.G.: 3D Slicer: A Platform for Subject-Specific Image Analysis,
Visualization, and Clinical Support, pp. 277–289. Springer New York, New York, NY (2014). URL
https://doi.org/10.1007/978-1-4614-7657-3_19
16. Matsumura, N., Ogawa, K., Ikegami, H., Collin, P., Walch, G., Toyama, Y.: Computed tomography
measurement of glenoid vault version as an alternative measuring method for glenoid version. Journal of
orthopaedic surgery and research 9(1), 17 (2014). URL https://doi.org/10.1186/1749-799x-9-17
17. Moineau, G., Levigne, C., Boileau, P., Young, A., Walch, G., French Society for Shoulder and Elbow
(SOFEC): Three-dimensional measurement method of arthritic glenoid cavity morphology: feasibility and
reproducibility. Orthopaedics and traumatology, surgery and research : OTSR 98(6 Suppl), S139—45 (2012).
URL https://doi.org/10.1016/j.otsr.2012.06.007
18. Nyffeler, R.W., Jost, B., Pfirrmann, C.W., Gerber, C.: Measurement of glenoid version: conventional
radiographs versus computed tomography scans. Journal of shoulder and elbow surgery 12(5), 493–496
(2003)
19. Olafsdottir, A., Thompson, S.: Scikit-surgeryglenoid (2022). URL
https://doi.org/10.5281/zenodo.5901818
20. Schneider, C., Thompson, S., Totz, J., Song, Y., Allam, M., Sodergren, M., Desjardins, A., Barratt, D.,
Ourselin, S., Gurusamy, K., et al.: Comparison of manual and semi-automatic registration in augmented
reality image-guided liver surgery: a clinical feasibility study. Surgical endoscopy 34(10), 4702–4711 (2020).
URL https://doi.org/10.1007/s00464-020-07807-x
21. Schroeder, W., Martin, K.M., Lorensen, W.E.: The Visualization Toolkit (2Nd Ed.): An Object-oriented
Approach to 3D Graphics. Prentice-Hall, Inc., Upper Saddle River, NJ, USA (1998)
22. Schroeder, W.J., Ibáñez, L., Martin, K.M.: Software process: the key to developing robust, reusable and
maintainable open-source software. In: 2004 2nd IEEE International Symposium on Biomedical Imaging:
Nano to Macro (IEEE Cat No. 04EX821), pp. 648–651. IEEE (2004)
23. Shapey, J., Dowrick, T., Delaunay, R., Mackle, E.C., Thompson, S., Janatka, M., Guichard, R.,
Georgoulas, A., Pérez-Suárez, D., Bradford, R., Saeed, S.R., Ourselin, S., Clarkson, M.J., Vercauteren, T.:
Integrated multi-modality image-guided navigation for neurosurgery: open-source software platform using
state-of-the-art clinical hardware. International journal of computer assisted radiology and surgery 16(8),
1347—1356 (2021). URL https://doi.org/10.1007/s11548-021-02374-5
24. Shukla, D.R., McLaughlin, R.J., Lee, J., Nguyen, N.T.V., Sanchez-Sotelo, J.: Automated
three-dimensional measurements of version, inclination, and subluxation. Shoulder & elbow 12(1), 31—37
(2020). URL https://doi.org/10.1177/1758573218825480
25. Sprowls, G.R., Wilson, C.D., Stewart, W., Hammonds, K.A.P., Baruch, N.H., Ward, R.A., Robin,
B.N.: Intraoperative navigation and preoperative templating software are associated with increased glenoid
baseplate screw length and use of augmented baseplates in reverse total shoulder arthroplasty. JSES
international 5(1), 102—108 (2021). URL https://doi.org/10.1016/j.jseint.2020.09.003
26. Thompson, S., Dowrick, T., Ahmad, M., Opie, J., Clarkson, M.J.: Are fiducial registration error and
target registration error correlated? scikit-surgeryfred for teaching and research. In: Medical Imaging
2021: Image-Guided Procedures, Robotic Interventions, and Modeling, vol. 11598, p. 115980U. International
Society for Optics and Photonics (2021). URL https://doi.org/10.1117/12.2580159
27. Thompson, S., Dowrick, T., Ahmad, M., Xiao, G., Koo, B., Bonmati, E., Kahl, K., Clarkson, M.J.:
Scikit-surgery: compact libraries for surgical navigation. International journal of computer assisted radiology
and surgery 15(7), 1075—1084 (2020). URL https://doi.org/10.1007/s11548-020-02180-5
28. Thompson, S., Dowrick, T., Xiao, G., Ramalhinho, J., Robu, M., Ahmad, M., Taylor, D., Clarkson,
M.J.: Snappysonic: An ultrasound acquisition replay simulator. Journal of Open Research Software 8(1)
(2020). URL http://doi.org/10.5334/jors.289
29. Wong, B.: Points of view: Color blindness. Nature methods 8, 441 (2011). URL
https://doi.org/10.1038/nmeth.1618